
You have had a blood test, and the report has come back with numbers against LDL, HDL, triglycerides, and total cholesterol. Perhaps your doctor has said your cholesterol is ‘a little high’ and mentioned something about medication. Or perhaps everything looked fine but you want to understand what you are actually being tested for.
Cholesterol is one of the most important — and most misunderstood — risk factors for heart disease. In this guide, I will break down exactly what each number means, what targets you should be aiming for, what causes abnormal levels, and what you can do about them.
What Is Cholesterol?
Cholesterol is a waxy, fat-like substance found in every cell of the body. It is essential for life — your body uses it to build cell membranes, produce hormones (including oestrogen and testosterone), make vitamin D, and synthesise bile acids that help digest fat.
Most of the cholesterol in your body is produced by your liver — dietary cholesterol from food contributes, but less than many people assume. The problem arises not with cholesterol itself but with how it is transported through the bloodstream and where it ends up.
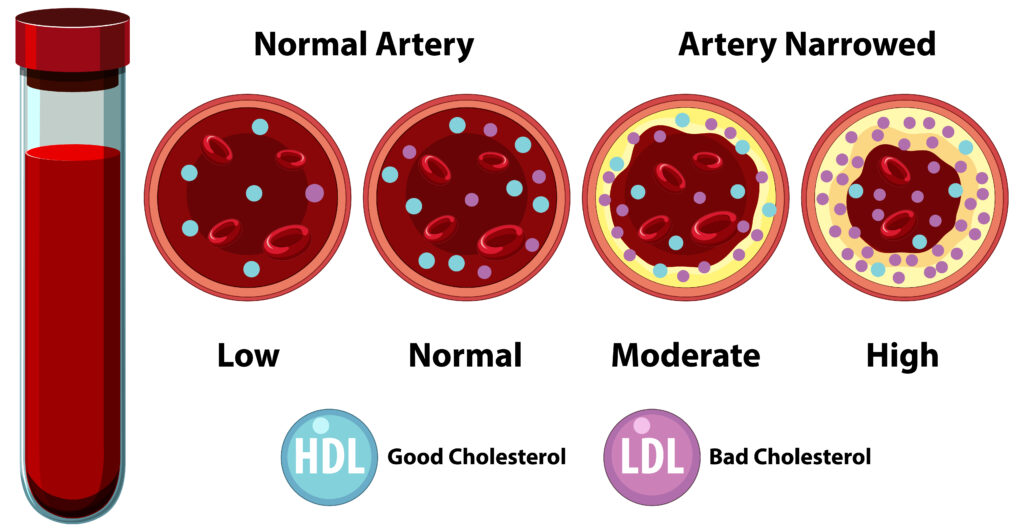
Cholesterol cannot dissolve in blood. It is carried by proteins called lipoproteins — and it is the type of lipoprotein carrying the cholesterol that determines whether it is protective or damaging. This is the origin of the ‘good’ and ‘bad’ cholesterol distinction.
| Key point: Cholesterol itself is not the enemy — it is essential. The danger lies in elevated LDL cholesterol, which deposits in artery walls and causes blockages. The goal of treatment is not to eliminate cholesterol but to optimise its distribution between protective and harmful forms. |
LDL: The ‘Bad’ Cholesterol
Low-Density Lipoprotein (LDL) is the primary carrier of cholesterol from the liver to the body’s tissues. When LDL levels are too high, excess cholesterol accumulates in the walls of arteries — a process that begins the formation of plaques (atherosclerosis).
Over time, these plaques narrow the arterial channel, reducing blood flow to the heart and other organs. When a plaque ruptures, it triggers a blood clot that can completely block the artery — causing a heart attack or stroke.
LDL targets depend on your overall risk level:
- General population with no risk factors: LDL below 130 mg/dL is acceptable; below 100 mg/dL is optimal
- Patients with diabetes, hypertension, or smoking history: LDL below 100 mg/dL
- Patients with established heart disease, prior heart attack, or stroke: LDL below 70 mg/dL
- Very high-risk patients (recurrent cardiac events, familial hypercholesterolaemia): LDL below 55 mg/dL
| Why LDL targets differ by risk: The same LDL level of 110 mg/dL may be acceptable for a healthy 35-year-old with no risk factors but dangerously high for a 60-year-old who has already had a heart attack. LDL targets are always interpreted in the context of your overall cardiovascular risk profile — not as a universal number. |
HDL: The ‘Good’ Cholesterol
High-Density Lipoprotein (HDL) works in the opposite direction to LDL. It collects excess cholesterol from the arterial walls and transports it back to the liver for processing and elimination — a process called reverse cholesterol transport.
Higher HDL levels are associated with lower cardiovascular risk. An HDL above 60 mg/dL is considered cardioprotective. An HDL below 40 mg/dL in men, or below 50 mg/dL in women, is a significant risk factor for heart disease — even if total cholesterol appears normal.
How to raise HDL naturally:
- Regular aerobic exercise — one of the most effective HDL boosters; 30 minutes of brisk walking or cycling five days a week can raise HDL by 5–10%
- Quit smoking — smoking actively suppresses HDL; stopping raises it within weeks
- Moderate alcohol (if applicable) — moderate consumption (1 drink/day) is associated with slightly higher HDL, though this must be weighed against other health risks
- Reduce trans fats — trans fats simultaneously raise LDL and lower HDL, a uniquely harmful combination
- Increase monounsaturated fats — olive oil, avocados, and nuts raise HDL
- Lose excess weight — even modest weight loss improves HDL
| Limitation of HDL as a target: Despite HDL’s protective association, clinical trials of medications designed to artificially raise HDL have been disappointing — raising HDL with drugs does not consistently reduce heart disease risk. The protective effect appears to come from functional HDL that works correctly, not simply a high number. Focus on lifestyle changes to raise HDL naturally. |
Triglycerides: The Overlooked Number
Triglycerides are the most common type of fat in the body. After you eat, your body converts unused calories into triglycerides, which are stored in fat cells and released between meals for energy. Persistently elevated triglycerides — a condition called hypertriglyceridaemia — are an independent risk factor for cardiovascular disease, particularly when accompanied by low HDL and high LDL.
What raises triglycerides?
- Excess refined carbohydrates and sugar — the primary dietary driver; white rice, maida, sugary drinks, and sweets convert rapidly to triglycerides
- Alcohol — even moderate drinking raises triglycerides significantly in susceptible individuals
- Obesity, particularly abdominal fat
- Type 2 diabetes and insulin resistance
- Hypothyroidism (underactive thyroid)
- Certain medications including beta-blockers, steroids, and some diuretics
Triglycerides above 500 mg/dL carry a specific additional risk: acute pancreatitis (severe inflammation of the pancreas). This is a medical emergency and requires urgent treatment.
| When triglycerides are very high: A triglyceride level above 500 mg/dL requires urgent medical attention regardless of other cholesterol numbers. Your cardiologist will recommend a combination of prescription medication (fibrates or high-dose omega-3), strict dietary sugar and alcohol restriction, and treatment of any underlying cause such as uncontrolled diabetes. |
Total Cholesterol: A Useful but Incomplete Number
Total cholesterol is the sum of LDL, HDL, and a portion of triglycerides. While it is the number most people are familiar with, it is actually the least informative on its own. A total cholesterol of 220 mg/dL could represent two very different risk profiles:
- A patient with high LDL (160), low HDL (30), and high triglycerides (150) — very high risk
- A patient with low LDL (90), high HDL (110), and normal triglycerides (100) — very low risk
This is why a full lipid panel — measuring LDL, HDL, triglycerides, and total cholesterol separately — is essential. Never make treatment decisions based on total cholesterol alone.
| Non-HDL cholesterol: An increasingly used and reliable measure is non-HDL cholesterol: total cholesterol minus HDL. This captures all the harmful cholesterol-carrying particles. A non-HDL below 130 mg/dL is generally the target for most adults. Ask your cardiologist for this calculation if it is not already on your report. |
Your Complete Cholesterol Reference Guide
| Measure | Optimal | Borderline | High Risk | Unit |
| Total Cholesterol | Less than 200 | 200–239 | 240 or above | mg/dL |
| LDL (Bad) | Less than 100 (less than 70 if high-risk) | 100–129 | 130 or above | mg/dL |
| HDL (Good) — Men | 60 or above | 40–59 | Less than 40 | mg/dL |
| HDL (Good) — Women | 60 or above | 50–59 | Less than 50 | mg/dL |
| Triglycerides | Less than 150 | 150–199 | 200 or above | mg/dL |
| Non-HDL Cholesterol | Less than 130 | 130–159 | 160 or above | mg/dL |
What Causes High Cholesterol?
Elevated cholesterol — particularly high LDL — results from a combination of genetic and lifestyle factors:
Lifestyle causes (modifiable):
- Diet high in saturated fats (red meat, full-fat dairy, ghee in excess, coconut oil) and trans fats (vanaspati, processed baked goods)
- Physical inactivity — exercise actively lowers LDL and raises HDL
- Obesity — excess body fat increases LDL production and decreases HDL
- Smoking — lowers HDL and damages artery walls, making LDL deposits more likely
- Excessive alcohol — raises triglycerides
Genetic causes (non-modifiable):
- Familial hypercholesterolaemia (FH) — a genetic condition affecting 1 in 250 people that causes LDL to be dramatically elevated from birth, often requiring medication from a young age regardless of lifestyle
- Family history of early heart disease — suggests genetic predisposition to abnormal lipid metabolism
- Hypothyroidism, kidney disease, and liver disease can all secondarily raise cholesterol
| Familial hypercholesterolaemia: If your LDL is above 190 mg/dL despite a healthy lifestyle, or if close relatives had heart attacks before age 55 (men) or 65 (women), ask your cardiologist about testing for familial hypercholesterolaemia. It is vastly underdiagnosed and, if missed, leads to heart attacks in otherwise healthy young people. |
Diet and Exercise to Improve Your Cholesterol
Lifestyle intervention is the foundation of cholesterol management. Depending on your baseline numbers and overall risk, diet and exercise alone may be sufficient — or may reduce the dose of medication needed.
Dietary changes with the strongest evidence:
- Replace saturated fats with unsaturated fats — switch from butter and ghee to olive oil or mustard oil; replace red meat with fish, legumes, and tofu
- Increase soluble fibre — oats, barley, dal, psyllium husk (isabgol), and fruits like guava and pear actively bind cholesterol in the gut and reduce LDL by 5–10%
- Eat more plant sterols — found in fortified foods and naturally in nuts, seeds, and vegetable oils; they block cholesterol absorption
- Reduce refined carbohydrates and sugar to lower triglycerides
- Eat fatty fish twice a week or take prescription omega-3 if triglycerides are very high
- Include nuts daily — 30g of walnuts or almonds reduces LDL by approximately 5%
Exercise targets:
- 150 minutes of moderate aerobic exercise per week (e.g., brisk walking, swimming, cycling) lowers LDL by approximately 3–6% and raises HDL
- Resistance training 2 days per week provides additional lipid benefits
- Even small increases in physical activity from a sedentary baseline produce measurable cholesterol improvements
Statins and Other Medications: When Are They Needed?
Medication is recommended when lifestyle changes alone are insufficient to reach your LDL target — which is determined by your overall cardiovascular risk, not just the cholesterol number itself. Statins are the most widely prescribed and best-evidenced cholesterol-lowering medications in the world.
| Medication Class | Examples | How It Helps |
| Statins | Atorvastatin, rosuvastatin, pitavastatin | Most powerful LDL reducer; also stabilises plaque. First-line for most patients. |
| Ezetimibe | Ezetimibe (Ezetrol) | Blocks cholesterol absorption in the gut. Often combined with a statin for added LDL reduction. |
| PCSK9 inhibitors | Evolocumab, alirocumab (injectable) | Dramatically lower LDL by up to 60%. Used for familial hypercholesterolaemia or statin intolerance. |
| Fibrates | Fenofibrate, gemfibrozil | Primarily lower triglycerides and raise HDL. Used when triglycerides are very high. |
| Omega-3 (prescription) | Icosapentaenoic acid (Vascepa) | High-dose EPA reduces triglycerides and cardiovascular events in high-risk patients. |
| Bile acid sequestrants | Cholestyramine, colesevelam | Reduce LDL by binding bile acids in the gut. Less commonly used now. |
| Are statins safe for long-term use? Statins are among the most extensively studied medications in medical history, with decades of safety data from millions of patients. Serious side effects are rare. Muscle pain (myalgia) occurs in a small percentage of patients and usually resolves with dose adjustment or switching to a different statin. Liver damage from statins is extremely rare. The cardiovascular benefits in high-risk patients far outweigh the risks for the vast majority of people who need them. |
Frequently Asked Questions
Does high cholesterol cause symptoms?
Almost never — which is what makes it so dangerous. High LDL cholesterol is completely symptomless until it has caused significant arterial disease. The only exception is familial hypercholesterolaemia, which can cause visible fatty deposits called xanthomas around the tendons and eyes. For everyone else, a blood test is the only way to know. This is why regular lipid screening is essential.
Can I stop my statin if my cholesterol comes down?
No — and this is one of the most common and dangerous mistakes patients make. Statins lower cholesterol while you take them, not permanently. If you stop, your LDL returns to its previous level within weeks. Statins also provide benefits beyond cholesterol reduction — including plaque stabilisation and anti-inflammatory effects. Unless your cardiologist advises otherwise, statins for established heart disease are lifelong medications.
How often should I get my cholesterol checked?
Adults with normal levels and no risk factors: every 4–5 years from age 20 is reasonable. Adults with elevated levels, risk factors, or on treatment: every 3–6 months until stable, then annually. After starting or changing a statin, a repeat lipid panel in 6–8 weeks confirms the medication is working as expected.
Is egg consumption bad for cholesterol?
This has been heavily debated. Current evidence suggests that for most healthy people, moderate egg consumption (up to one egg per day) does not significantly raise cardiovascular risk. Dietary cholesterol from eggs has less impact on blood LDL than saturated fat does. However, for patients with familial hypercholesterolaemia or established heart disease, it is prudent to limit egg yolks to 3–4 per week. As always, discuss with your cardiologist based on your specific risk profile.
The Bottom Line
Understanding your cholesterol report is not complicated — once you know what each number means and why it matters. LDL is the primary driver of arterial blockages and the main target of treatment. HDL protects the heart and should be maximised through lifestyle. Triglycerides reflect diet and metabolic health. Total cholesterol alone tells you very little without the breakdown.
The most important steps you can take are: get your full lipid panel checked regularly, know your numbers, and act on them appropriately — whether through diet, exercise, medication, or a combination of all three. High cholesterol is one of the most controllable cardiovascular risk factors. With the right management, it need not define your cardiac future.
| Get Your Lipid Panel Checked Today Our cardiologist will interpret your cholesterol numbers in the context of your full cardiovascular risk profile and recommend the right management plan for you. |